Purpose/Objective: In radiation therapy for uterine cervical cancer, three-dimensional image-guided brachytherapy (3D-IGBT) using magnetic resonance imaging (MRI) or computed tomography (CT) has shown promise for improving local control without increasing the risk of severe complications. Although MRI is the gold standard for 3D-IGBT for cervical cancer, its global application is still limited. Recent surveys on IGBT for cervical cancer demonstrated that CT is the most commonly used imaging modality for dose specification in clinical practice in Japan. Considering the fact that CT is a mainstay for 3D-IGBT in the majority of institutions, the resulting dose uncertainty from such CT-based CTV contouring must be minimized. Therefore, we conducted a multi-institutional study of CT-based CTVHR delineation in order to standardize 3D-IGBT application in regions where the availability of MRI with applicator in place is limited.
Material/Methods: A 15-member Japanese Radiation Oncology Study Group (JROSG) committee with expertise in gynecological radiation oncology initiated guideline development for CT-based CTVHR, based on a comprehensive literature review as well as clinical experience, in July 2014. Extensive discussions occurred during 4 face-to-face meetings as well as frequent e-mail communication until a consensus was reached.
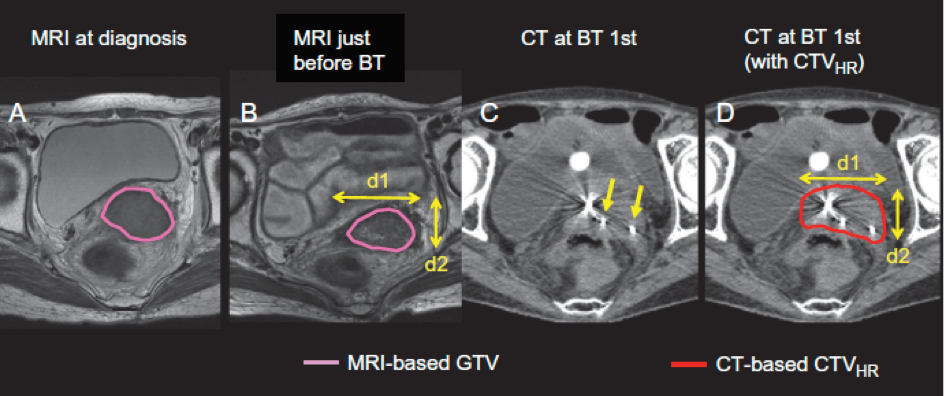
Results: The CT-based CTVHR boundaries are defined by each anatomical plane (cranial-caudal, lateral, or anterior-posterior) with or without tumor progression beyond the uterine cervix at diagnosis. Since the availability of MRI with applicator insertion for 3D planning is currently limited, T2-weighted MRI obtained at diagnosis and just before brachytherapy without applicator insertion is used as a reference to accurately estimate the tumor size and topography. Furthermore, utilizing information from clinical examinations performed both at diagnosis and brachytherapy is strongly recommended. The first version was reviewed by 2 external advisors; the value of MRI and limitations of CT in 3D-IGBT for cervical cancer were updated based on discussions between the external advisors and JROSG members. Finally, the revised recommendations were completed and approved by all members in June 2016.
Conclusions: We develop recommendations for contouring computed tomography (CT)-based high-risk clinical target volume (CTVHR) for three-dimensional image-guided brachytherapy (3D-IGBT) for cervical cancer. Our recommendation was adopted in the JASTRO Guidelines for Radiotherapy Treatment Planning in 2020. We initiated a comparison study for contouring CTVHR between CT- and MR-based brachytherapy. In addition, a multi-center clinical study using this recommendation is on-going at eight institutions with limited availability of MRI for 3D treatment planning.