A total
of 65 fractions were evaluated. Average residual errors were 2.83 (SD: 2.63) mm
and 0.62 (SD: 0.88) mm with the Body and Mask approaches. A total of
130 plan recalculations were performed. Following the deformation, visual
inspection showed good overall results and the Jacobian remained within
reasonable limits (Figure 1) confirming a plausible deformation for dose deformation
and accumulation.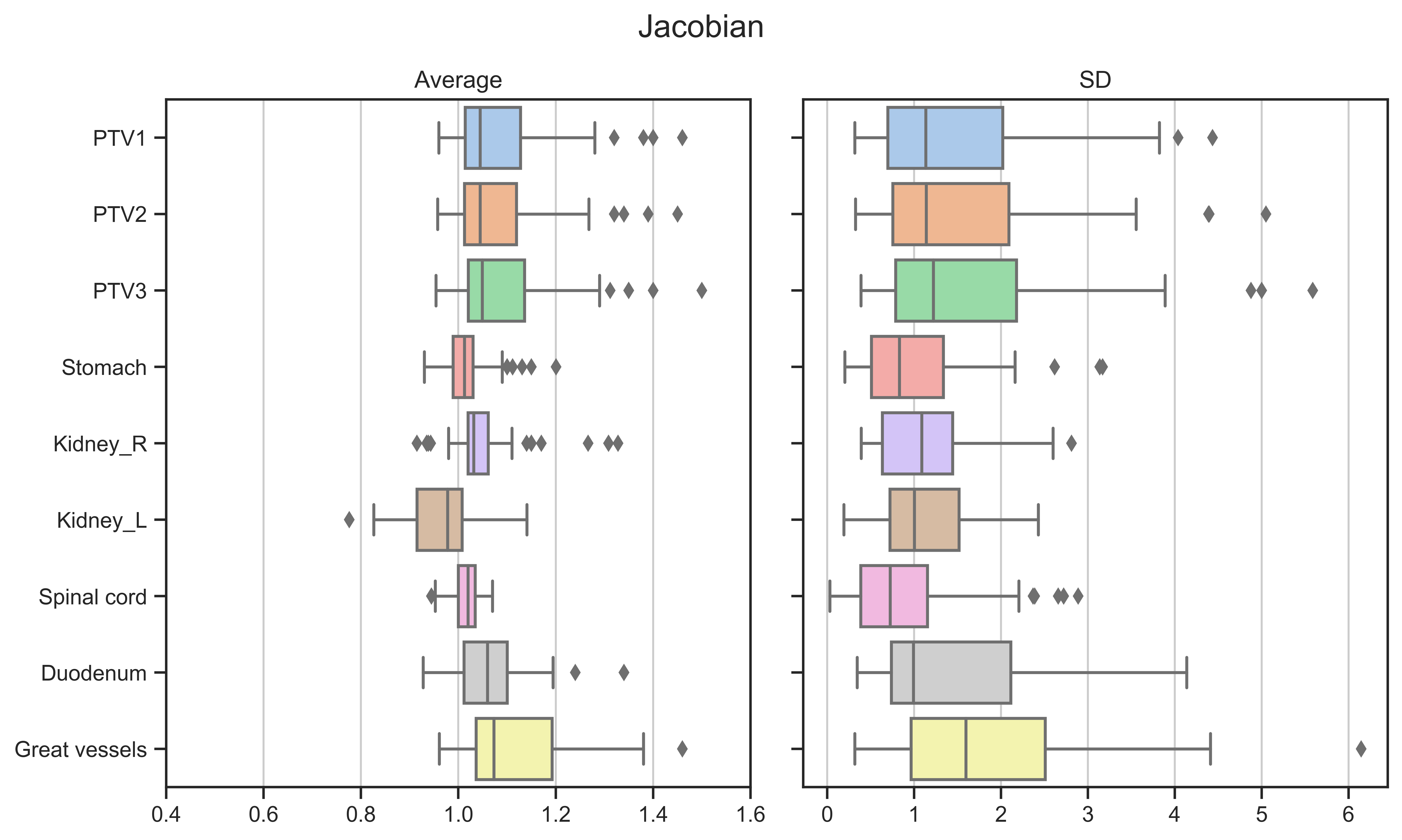
Figure 1. Average and SD of the Jacobians
for PTVs and OARs.
Daily dose coverage for the target volumes were maintained. The relevant
OARs constraints were also respected without major deviation from the planning
values, while no significant differences were found between the Body
or Mask
based processing (Figure 2). Accumulated dose remained
comparable to the planned one as well.
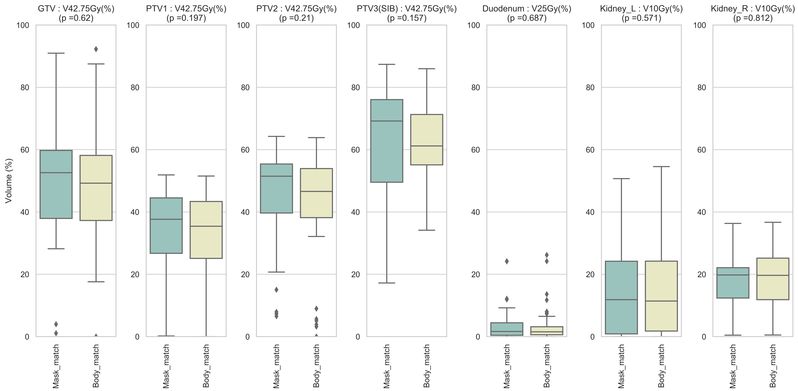
Figure 2. Daily DVH parameters using Mask and Body based deformation.