To
reduce the beam-on time, we increased the beam current reaching the patient by
developing new beam optics for PSI’s PROSCAN beamline and Gantry 2.
Experimentally we obtained up to factor 5 higher beam current transmission. A
more efficient tuning also achieved a factor 25 higher transmission but
resulted in 1.5 times larger pencil-beam size at the patient.
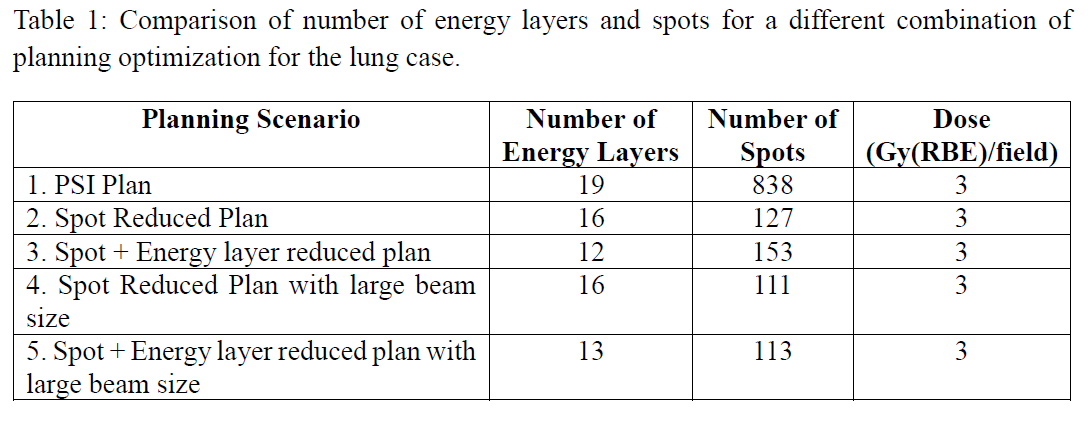
To
reduce the dead time between the spots, we used spot reduced plan optimization
[1]. This technique reduces the number of spots by 85% compared to the in-house
clinical planning system for the lung case considered. Adding an energy layer
reduction algorithm can further lower the dead time, by reducing the energy
layers by 37% compared to the PSI plan. As such, we planned the same case using
five different scenarios, based on three different treatment planning
optimization methods (Table 1).
Scenarios
1-3 were delivered with both the clinical and improved optics if PSI Gantry 2,
whereas for scenarios 4-5 (with larger beam sizes and higher transmissions), we
used only the improved optics. For all scenarios, we extracted treatment times,
due to both beam-on time and dead time, from the log-files.